CTP-Free Early Stroke Lesion Segmentation from NCCT and CTA
About

Summary
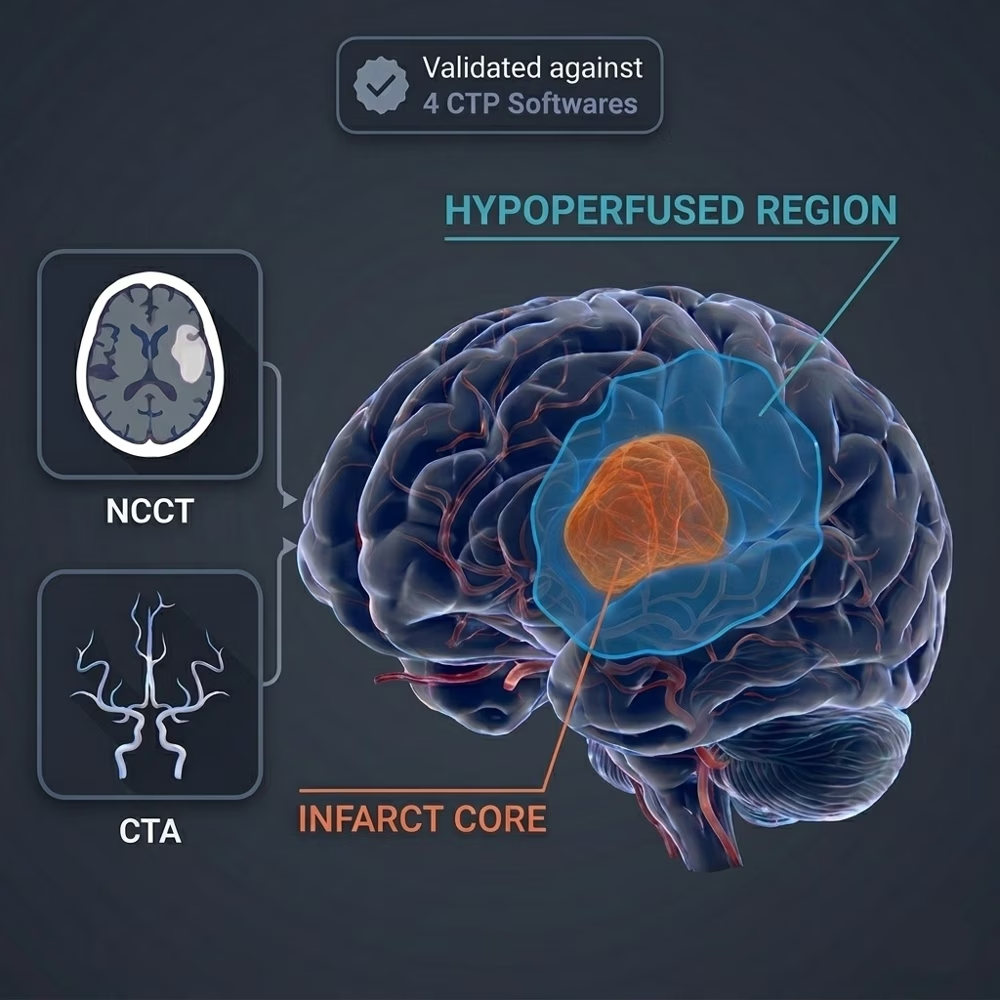
In acute ischemic stroke, the infarct core and hypoperfused regions are key indicators for assessing and prognosticating patients. However, these early ischemic lesions are not easily visible on CT scans. Consequently, they are now typically estimated with computed tomography perfusion (CTP). However, CTP is not always available in all medical centers and for all patients. Noncontrast CT (NCCT) and CT angiography (CTA) on the other hand, are much more widely available. Therefore, we created an algorithm to segment the early ischemic region from baseline NCCT and CTA.
TLDR; Our algorithm takes baseline NCCT and CTA as input, and returns the infarct and hypoperfused region.
For more information about the algorithm, please refer to: Estimation of Acute Infarct Core and Hypoperfused Region from Baseline Noncontrast Computed Tomography and Computed Tomography Angiography Scans of Patients with Ischemic Stroke.
Mechanism
All of our models are 3D nnU-Net networks. They are trained on early baseline CT scans as input. The ground truth that was used for training was obtained from a commercially available and CE certified and FDA approved CTP software, StrokeViewer (Nicolab, Amsterdam, The Netherlands). We tested our model against four different commercially available CTP software.
The NCCT + CTA model is our primary, validated algorithm and provides the highest performance. While we include fallback options for NCCT-only or CTA-only inputs, they do not perform as well as the dual-modality version. Users should consult the paper to understand the performance trade-offs before using these standalone options.
IMPORTANT NOTE: The NCCT and CTA scans should be registered to each other before being uploaded to this algorithm. For more information about medical image registration, you can consult this tutorial (or use any other image registration tool).
Interfaces
This algorithm implements all of the following input-output combinations:
| Inputs | Outputs | |
|---|---|---|
| 1 | ||
| 2 | ||
| 3 |
Validation and Performance
The results of comparing the NCCT+CTA model with StrokeViewer ground truth labels are shown in the table. Numbers in parenthesis are 95%CI. For further results including the validation of the single modality models and comparison with 4 different CTP software, please refer to our paper.
| Region | Dice Score | Surface Dice | Volumetric Diff (mL) |
|---|---|---|---|
| Infarct Core | 0.45 (0.39–0.50) | 0.52 (0.46 to 0.57) | -9.3 mL (−12.5 to −6.1) |
| Hypoperfused Region | 0.66 (0.62–0.69) | 0.63 (0.59 to 0.67) | -12.9 mL (−21.1 to −4.7) |
Uses and Directions
This algorithm was developed for research purposes only. Please cite our paper if you are using this algorithm for a publication.
Warnings
-
The NCCT and CTA scans should be registered to each other before being uploaded to this algorithm. For more information about medical image registration, you can consult this tutorial (or use any other image registration tool).
-
The NCCT + CTA model is our primary, validated algorithm and provides the highest performance. While we include fallback options for NCCT-only or CTA-only inputs, they do not perform as well as the dual-modality version. Users should consult the paper to understand the performance trade-offs before using these standalone options.
Common Error Messages
"The input images are not registered, they have different shapes": Make sure the NCCT and CTA scans are registered to each other.